- +91 9777668320
- hr.aiveer@gmail.com
Frozen Shoulder is a condition where the shoulder capsule (group of ligaments enclosing the shoulder joint) becomes stiff and tight. Thick bands of tissue called adhesions develop in the shoulder capsule and for this reason Frozen Shoulder is also termed as Adhesive Capsulitis in medical terms.
- Pain – Shoulder pain that may worsen at night and disturb your sleep.
- Stiffness – Stiffness in the shoulder
- Limited or Restricted range of motion of the shoulder
There are typically 3 stages:
1. Stage 1: FREEZING
- Can last between 6 weeks to 9 months
- Slow onset of shoulder pain
- Pain starts worsening
- Stiffness in the shoulder joint gradually starts
- 2. Stage 2: FROZEN
- Can last between 4-12 months
- Shoulder pain gradually improves
- Stiffness continues to worsen that makes it hard to perform everyday activities.
- 3. Stage 3: THAWING
- Can last between 6 months to many years
- One may be able to move their shoulder & perform daily activities
- But studies have shown that over 20% of people suffering from Frozen Shoulder may develop long term limitations of Range of Motion (ROM) that may last upto 10 years.
No, surgery is not always necessary for a frozen shoulder (also known as adhesive capsulitis). Most cases of frozen shoulder can be managed with non-surgical treatments. If you need surgery, it is normally performed during the frozen phase of the condition.The surgeon will use arthroscopy (keyhole surgery), making small incisions around the shoulder joint and inserting an arthroscope (a thin, pencil-sized instrument). The aim is to stretch and release the stiffened joint capsule, breaking down scar tissue.
A frozen shoulder normally improves by itself, but this can take up to three years in some cases and often doesn’t completely resolve. The freezing stage, described above, can last between 6 and 9 months, the frozen stage between 4 and 12 months, and the thawing stage from 6 to 2 years. In the meantime, you can have treatments to help relieve the symptoms and speed up your recovery.
How can I cure my frozen shoulder quickly?
A: For quick relief
- Apply hot and cold compresses daily to reduce mild pain and discomfort.
For long-term relief
- Physiotherapy
- Home-based exercises, as these can help to improve your range of motion.
Examples of home-based exercises include:
- External rotation passive stretches
- Forward flexions in the spine position
- Crossover arm stretches

A: The doctor will refer you to a physical therapist who will teach you several exercises to stretch your joints and strengthen your muscles. These exercises involve gentle and circular movements that may go upanddown or sidetoside.
One such exercise is the internal rotation stretch, which you can do with a towel:
- Drape a bath towel over your stiff shoulder and hold one end of the towel in your hand at shoulder level.
- Reach your other hand behind your back and grab the other end of the towel.
- Pull the towel up your back until you feel a stretch in your shoulder.
- Hold the stretch for 15 seconds.
- Repeat this exercise 10 times.
- After your stretches and exercises, you should ice your joints.
Studies have shown that patients with diabetes are more likely to get shoulder disorders such as frozen shoulder and rotator cuff disease.
Treatment for a frozen shoulder is to
- Relieve pain
- Restore movement and shoulder function.
- Physiotherapy
- Home- exercise are the first-line treatment for all stages of Frozen shoulder.
- Anti-inflammatory medications and glenohumeral joint corticosteroid injections.[53]
Most patients with adhesive capsulitis are treated nonoperatively; more than 90% respond to conservative interventions to control pain and restore motion. Invasive options for refractory cases include extracorporeal shockwave therapy, manipulation under anesthesia, hydro dilatation (hydrodistension), and selective arthroscopic capsular release.
Steroids are powerful drugs, which, used appropriately, can be very helpful, but, used inappropriately, can cause problems. In general, we limit steroid injections to a maximum of three per joint - if a patient is not better after three injections, they are unlikely to get better with further injections. Repeated injections risk damaging the rotator cuff tendons. The risks of any injection include infection, but this is a very rare complication. The majority of the steroid stays locally and do not cause generalized steroid side effects, though diabetics may notice their blood sugar control is affected by the injection. So, don’t take steroids unless and until advised by your doctor.
Muscle stiffnessis a feeling of tightness or resistance in the muscles that can make movement more difficult or uncomfortable. It can range from mild and temporary to more severe or chronic.
Muscle stiffness can occur due to several reasons, including:
- Due to a disease of the muscles (myopathy) or nerve and muscle issues (neuromuscular disorders)
- Sleeping in an awkward position
- Sitting at a computer all day
- Overuse, intense exercise, or an unfamiliar activity can cause muscle soreness and stiffness, often called delayed onset muscle soreness (DOMS).
- Strains, sprains, or muscle tears
- Lack of fluids or imbalanced electrolytes
- Poor posture, especially from sitting for long periods
- Ageing
- Medical Conditions like Arthritis, Fibromyalgia, Multiple sclerosis, and Parkinson’s disease
- Stretching exercises can help loosen stiff muscles
- Staying hydrated
- Consuming enough calcium and magnesium and some nutritional supplements can also help prevent muscle stiffness.
- Applying heat or cold therapy to the affected area can help to reduce muscle stiffness and discomfort. Heat can relax tight muscles, while cold can help to reduce inflammation.
- Regular exercise can help strengthen and stretch muscles, reducing stiffness and discomfort.
Seek medical attention if:
- The stiffness is severe or lasts for more than a few days.
- You experience other symptoms like swelling, bruising, or a visible deformity.
- The stiffness is accompanied by numbness, weakness, or difficulty moving.
- It follows an injury (especially if you suspect a tear or sprain).
- The stiffness is recurrent or chronic and not related to exercise.
Yes, muscle stiffness particularly 24 to 48 hours after a workout, is common and is referred to as delayed onset muscle soreness (DOMS). It happens due to micro-tears in the muscle fibres and the subsequent healing process. However, if the stiffness is extreme or doesn't improve with rest, it may indicate overtraining or an injury.
Yes, poor posture, especially when sitting for long periods, can lead to muscle stiffness in the neck, back, and shoulders. Hunching over can put undue muscle stress, leading to tightness and discomfort. Regular stretching and correcting your posture can help alleviate this.
Muscle stiffness refers to tightness or rigidity in the muscle, often without pain, and is usually the result of overuse, tension, or injury.
Muscle cramping is a sudden, involuntary contraction of a muscle that causes intense pain, typically due to dehydration, low electrolytes, or muscle fatigue.
Yes, stress can contribute to muscle stiffness. People tend to tense their muscles when stressed, especially in areas like the neck, shoulders, and back. Chronic stress can lead to prolonged muscle tension and stiffness.
Joint replacement is a surgical procedure where a damaged joint is replaced with a prosthetic implant. It is done to relieve pain and improve function in patients with severe joint arthritis or injury. The most common joints that are replaced are the hip and knee, but other joints like the shoulder, elbow, and ankle can also be replaced.
Joint replacement is typically recommended when other treatments (like medications, physical therapy, and lifestyle changes) no longer provide relief from pain or improve function. It's often considered when severe arthritis, injury, or other conditions cause chronic pain and disability, affecting daily activities like walking or climbing stairs.
- Total joint replacement: The entire joint is replaced, such as hip replacement or knee replacement replacements.
- Resurfacing: Only the joint surface is replaced (like hip resurfacing).
- Revision joint replacement: A second surgery to replace or repair an earlier joint implant that has worn out or failed.
Joint replacements can last 15 to 20 years or longer, but their lifespan depends on factors like age, activity level, and the type of implant used. Re-operation may be required if the implant wears out or fails.
- Infection at the incision site or deep within the joint.
- Blood clots, especially in the legs.
- Implant failure or wear over time.
- Dislocation of the joint (particularly with hip replacement).
- Nerve or blood vessel injury during surgery.
However, the overall risk of serious complications is relatively low with advanced technique surgery.
Yes, the patient needs to stay in the hospital after surgery for a few days to a week, depending on the type of joint and your overall health condition. Some patients may undergo a same-day discharge or shorter stay, especially with minimally invasive techniques.
- Total joint replacement involves replacing both the femoral (thigh bone) and acetabular (hip socket) components in the case of a hip, or the femur, tibia, and sometimes the patella in knee replacement.
- Partial joint replacement means replacing only a portion of the joint. This is most commonly done in the knee if only one side of the knee is affected.
- Allowing people to return to daily activities without constant discomfort.
- Improved mobility helps with tasks like walking, climbing stairs, and sitting comfortably.
- Improvement in quality of life.
- The ability to drive depends on your recovery progress and which joint was replaced.
- Hip and knee replacements, you will need to wait until you have regained sufficient mobility and strength and are no longer taking pain medications that could impair driving.
- It’s usually safe to drive after 4 to 6 weeks, but this varies.
Yes, physical therapy can be very effective in managing osteoarthritis. A physical therapist can guide you through exercises to strengthen muscles around the affected joint, which helps improve joint stability and reduce pain. Stretching and mobility exercises may also improve flexibility and reduce stiffness.
Excess weight increases the stress placed on weight-bearing joints like the knees and hips, accelerating the wear and tear of cartilage. Losing weight can reduce the load on these joints, which helps alleviate pain and prevent further damage. Maintaining a healthy weight is one of the most effective strategies for managing Osteoarthritis.
Excess weight increases the stress placed on weight-bearing joints like the knees and hips, accelerating the wear and tear of cartilage. Losing weight can reduce the load on these joints, which helps alleviate pain and prevent further damage. Maintaining a healthy weight is one of the most effective strategies for managing Osteoarthritis.
While osteoarthritis cannot always be prevented, certain measures can reduce your risk:
- Low-impact activities like swimming, cycling, and walking strengthen muscles and help maintain joint function.
- Reducing excess weight reduces stress on joints, particularly weight-bearing ones.
- Take breaks during repetitive activities to prevent joint strain.
- Using proper technique during physical activities and wearing supportive footwear can help prevent OA.
- Heat can relax stiff muscles,
- Cold therapy can reduce swelling and inflammation.
- Glucosamine, chondroitin, and omega-3 fatty acids may help reduce inflammation and support joint health, though evidence for their effectiveness is mixed.
- Turmeric and ginger both have anti-inflammatory properties that may help with Osteoarthritis pain and stiffness.
- Acupuncture helps manage pain and improve joint mobility.
- Your joint pain or stiffness worsens or persists.
- You notice swelling or tenderness that doesn’t go away.
- Your symptoms interfere with daily activities.
- You experience a significant decrease in your joint’s range of motion.
While OA is more common in older adults, it can affect younger individuals, especially if they have had joint injuries or certain genetic conditions. This is sometimes referred to as juvenile osteoarthritis, but it is rare and typically occurs after significant trauma or in those with congenital joint deformities.
- Engage in low-impact activities to strengthen muscles and keep the joints flexible.
- Maintain a healthy weight to reduce stress on joints.
- Use over-the-counter pain relievers as directed by the physician, apply heat or cold therapy, and consider using supportive devices like braces or splints.
- Avoid movements that strain your joints, and use assistive devices when necessary.
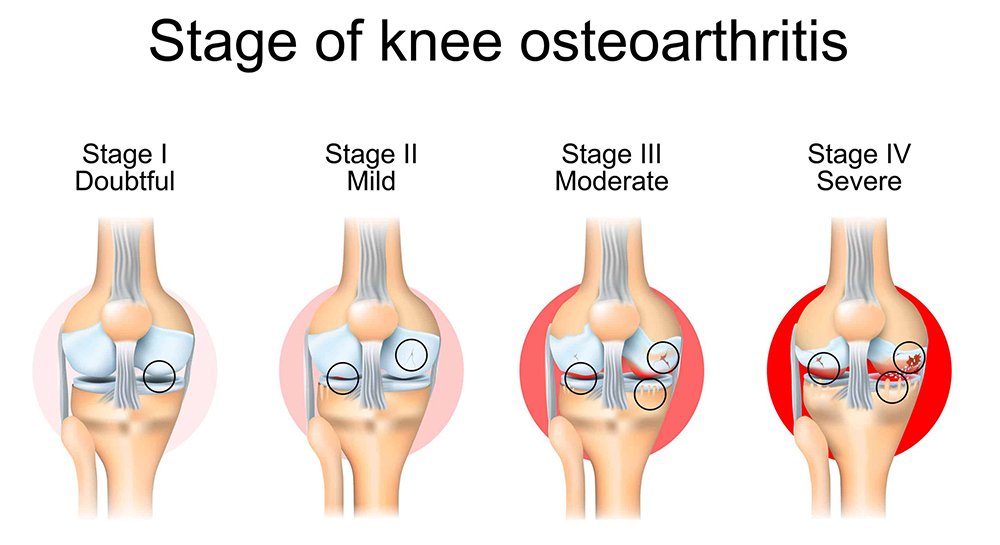
Stage 1: Minor (Early Stage)
There is minimal wear and tear on the cartilage. The cartilage begins to lose some of its elasticity and smoothness, but it remains thick and there is no significant damage. There may be very little or no pain or stiffness.
- Stage 2: Mild (Early Osteoarthritis)
Cartilage wear becomes visible, with thinning and small cracks or fissures forming in the cartilage. However, the joint is still able to function reasonably well.Pain and stiffness may begin to occur more frequently, especially after activity or at the end of the day. Joint movement might be slightly restricted, but most daily activities are still possible without major difficulty.
- Stage 3: Moderate (Advanced Osteoarthritis)
The cartilage is now damaged. The bones may begin to rub against each other, causing inflammation and pain.Pain becomes more constant and may be present even at rest. Joint stiffness is more pronounced, and the range of motion is more limited. Activities like walking, bending, or lifting may become difficult.
- Stage 4: Severe (End-Stage Osteoarthritis)
The cartilage is severely worn away, and there may be little to no cartilage left in the joint. The bones are rubbing against each other, causing pain, swelling, and inflammation.Pain is often constant and can be disabling, limiting mobility and making it difficult to perform even basic daily activities. Joint deformities may be present, and muscle weakness can develop due to reduced movement.